[Disclaimer: This is a personal story, the first of a series from doctors and other applicants explaining their perspectives. It is not medical advice or information published in the practice of medicine.]
Dr Peter Parry
MBBS, PhD, FRANZCP, Cert Child Adoles Psychiatry
Associate Professor*, Child & Adolescent Psychiatry
*views are own and do not necessarily reflect those of affiliated institutions
How I became an applicant in a Judicial Review to the Qld Supreme Court
I realise those friends, colleagues and anyone reading this who firmly believes in the ‘safe and effective’ message regarding the C19 vaccines might experience some cognitive dissonance with what is presented here. You may have an urge to stop reading now. But I politely request to please read with an open mind in the spirit of true scientific discourse and medical ethics.
Covid-19 has been a serious illness and fatal for some people, even now with Omicron, and protection and good treatment are important, which includes safe and effective vaccines.
I never thought I would find myself as an applicant to any court, let alone the Supreme Court of Queensland. The way I found myself appealing to the Supreme Court of Queensland for the overturning of the Hospital Employment Directive number 12 of 2021 (HED12/21) is as follows.
I graduated from medical school 40 years ago and in all that time have never had a single complaint about me presented to a medical board or AHPRA. In 34 years’ continuous clinical work in the public health services of South Australia and Queensland, with leave to work a couple of years in the British NHS, I had never once been subject to ‘disciplinary’ action until I was suspended, and now recently terminated, from my employment as a senior medical officer (consultant child & adolescent psychiatrist) with Qld Health.
The reason for this was declining to take the mRNA or adenovectorDNA novel technologies C19 vaccines of Pfizer, Moderna or AstraZeneca, which are still only provisionally approved by the TGA. Why did I choose my informed declination rather than ‘informed consent’ to these agents, that all Qld Health staff were mandated to take by the HED12/21 document?
Basically, because these are not normal vaccines.
The mRNA technology had been experimented with only in small clinical trials that never came to market. It had never been used for public vaccinations before December 2020. The adenovectorDNA technology has rarely been used. Their mechanism of action is to insert gene codes for the Wuhan variant SARS-CoV-2 spike protein into our cells, which then manufacture this foreign protein, that then extrudes from our cells to attract our lymphocytes (B cells and T cells) to stimulate an immune response.
The obvious question (to some of us anyway) was – “What if the mRNA gets away from the deltoid muscle and makes spike proteins in the brain, heart, bone marrow, ovaries, testes etc?” I actually asked a senior colleague in early 2021 this, he assured me the ‘Science’ at the time was it stays in the deltoid and all the mRNA dissolves within hours or a day or so.
However, I did my research and found that there was a risk of widespread biodistribution of the gene codes into cells in all body organs, including heart, brain, ovaries etc. (see below). This knowledge should have stopped the rollout, but it didn’t. It should have led to widespread public and scientific debate, but that was suppressed.
I wish to add at this point that I am not an ‘anti-vaxxer’ which, during this pandemic, has been used as a slur against anyone questioning authority by pointing to data that contradicts the prevailing orthodoxy. But Science and Medical Ethics are all about questioning prevailing paradigms and authorities. Science and ethical clinical practice thrive in an atmosphere of transparency and open vigorous debate about data and hypotheses. I ask you; do you think that open atmosphere has prevailed over the past 3 years?
In fact, I have had three doses of a C19 vaccine – Spikogen – produced by Prof Nikolai Petrovsky’s Flinders Uni affiliated company, www.vaxine.net, as part of a phase 3b/4 clinical booster trial in late 2022. On that basis I have been working as a locum in some interstate public health services. Spikogen has peer reviewed research supporting its efficacy and safety, it has been given to millions of people in Iran where its phase 3 clinical trial was conducted. Spikogen uses traditional protein-based antigen technology and according to my conversations with Prof Petrovsky, the spike protein has been deactivated from attaching or entering human cells by removal of two segments – the furin cleavage site and the receptor binding domain. Interestingly there have been no systemic adverse effects reported to Iranian pharmacovigilance authorities.
I also have natural immunity after contracting Covid-19 in April 2022, in my case a flu-like illness that kept me in bed for 3 days and somewhat fatigued for about 3 weeks. It was milder than past bouts of influenza in my experience. I’ve had repeated serious exposure to Covid positive patients, colleagues, friends, and family during my interstate public health system locum work and so far, not contracted it again.
But Qld Health determined that because Spikogen is not yet TGA provisionally approved, that it wouldn’t recognise this as valid for vaccination purposes. Therefore, I need to successfully challenge the HED12/21 to be reinstated.
I’m obviously just one of many and thank my fellow applicants and the large numbers of well-wishers supporting us. Thousands of Qld Health workers have been terminated from their jobs since October 2021.
Although sacked Qld Health staff have applied in the hundreds, nobody yet has managed reinstatement via the Queensland Industrial Relations Commission. The QIRC appears to avoid looking at evidentiary matters and rule only on procedural grounds, whether the policy rules were followed.
We hope, by bringing evidentiary material and expert witness testimonies before the Supreme Court, that the Justices will look at the evidence and rule in our favour. If successful, large numbers of experienced nurses, allied health, and doctors will be able to return to assist an overstretched Qld public health system.
Doctors Against Mandates apparent September 2022 victory
We have grounds for hope. In September 2022, about a week after 17 of us ‘Doctors Against Mandates’ had our affidavits and 5 expert witness reports submitted to Crown Law, the Qld State Govt revoked the Public Health Directive (PHD) of the Chief Health Officer (CHO) of March 2022. ‘Correlation does not prove causation’ but the timing was quite dramatic once the evidence due to be heard in the Supreme Court was in the hands of Crown Law. By revoking the PHD of the CHO, the case could not proceed though, and the evidence was not formally heard and decided upon in court.
The Qld Govt urged private practices to voluntarily follow the HED12/21 and keep mandates in place. Nonetheless, that allowed most of us to return to private practice where the private clinic decided not to follow the HED12/21. However, two of us, Dr Sally Johnston, and myself, remain unable (along with thousands of other Qld Health staff) to return to our Qld Health jobs because of the HED12/21. Others of us are still barred from jobs with private hospitals such as The Mater, but for legal cost reasons do not have standing to challenge the HED12/21 . For legal technical reasons, last year’s case against the PHD of the CHO had to proceed before this current case against the HED12/21.
For this second case dealing with the HED12/21, Dr Johnston and I have been joined as plaintiffs by Dr Charles McDonald, PhD, cardiac perfusionist, and Marita Forchert, RN. Both suffered C19 vaccine injuries and did not wish to proceed with second doses and had their jobs terminated by Qld Health. Many other staff would like to join us, but legal costs can escalate.
But let’s get to the crux of the matter – the Science and Ethics. This is what will count in the fullness of time, but hopefully earlier in the Supreme Court.
My past research into an overdiagnosis & overtreatment epidemic and medical ethics
My PhD covered an overdiagnosis and overmedication epidemic of bipolar disorder in very young children (including thousands of pre-schoolers and toddlers) in the USA. The epidemic was driven by several factors but central was the power of Big Pharma to influence research, medical discourse and education, guidelines committees, journals, and professional medical colleges. This was further fuelled by influencing the media and funding advocacy groups.
You can skim read it on the Flinders University Theses website. Regarding the issue of ‘trusting the Science’, read Chapter 4.2 from page 95 of the thesis, and look at appendix A11 and appendix D.
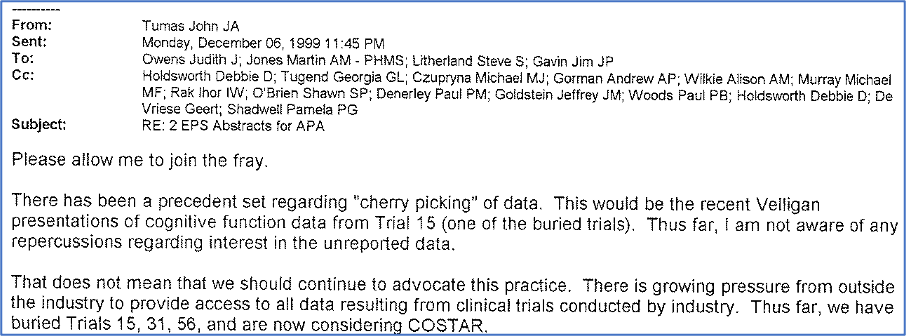
As you will see, part of my research involved reading through thousands of pages of internal pharmaceutical industry documents that were released after being subpoenaed by courts for charges of felonies. Did you know that Pfizer has over 40 convictions for over $10Billion, AstraZeneca over 20 convictions for $1.3Billion and Johnson&Johnson over $14Billion in criminal fines? Big Pharma as an industry have paid $95Billion in criminal fines and this does not include out of court class action settlements to aggrieved groups of litigating patients. If you have plenty of spare time you can see an early version of a lecture I give to mental health professionals.
So, from that research background I have a developed a ‘healthy scepticism’ of data and scientific papers where the data is subject to commercial confidentiality by manufacturers of the products. Researchers are sworn to non-disclosure agreements to not release data even if it is true data contradicting the false data published in journals. A former chief-editor of the British Medical Journal (BMJ) wrote an article “Medical Journals are an Extension of the Marketing Arm of Pharmaceutical Companies”. A 2003 meta-analysis comparing industry sponsored studies with completely independent studies found a 4-fold odds ratio of finding better safety and efficacy of a large range of medicines from studies by the sponsor of the drug than by truly independent studies of the same drug.
At present the FDA, TGA and other health regulators and authorities rely on Pfizer, Moderna, Johnson & Johnson and AstraZeneca for the ‘safe and efficacious’ clinical trials data. Plenty of research says the regulators need to do or fund their own independent studies.
So, when new products like the gene-based vaccines came along, I was cautious and did my research to inform my consent or declination of receiving them. In fact, I was not alone, a US survey in early 2021 found ‘vaccine hesitancy’ for the C19 vaccines was highest in medical PhD holders, followed by those without university degrees. It was lowest with those with basic university degrees who presumably have more unquestioning faith in what’s in the ‘prestigious’ journals. The depth of PhD research helps one realise the level of controversy and commercial interests in Medicine and Science
Pharmacokinetics of lipid-nanoparticle mRNA complexes
Wide biodistribution
Back to my question of early 2021: “Couldn’t the lipid-nanoparticles (designed to traverse cell membranes) carry the mRNA to cells around the body?”. A/Prof Byram Bridle, vaccinologist-virologist, from Canada and other scientists used Freedom of Information (FOI) laws to obtain the rat study biodistribution of Pfizer’s lipid-nanoparticles around the rats’ bodies after injection in their gluteal muscles. The Japanese Pharmaceuticals & Medical Devices Agency (PMDA), Japan’s version of the US Food & Drug Administration (FDA), released the data while the US FDA did not.
The results should be deeply concerning.
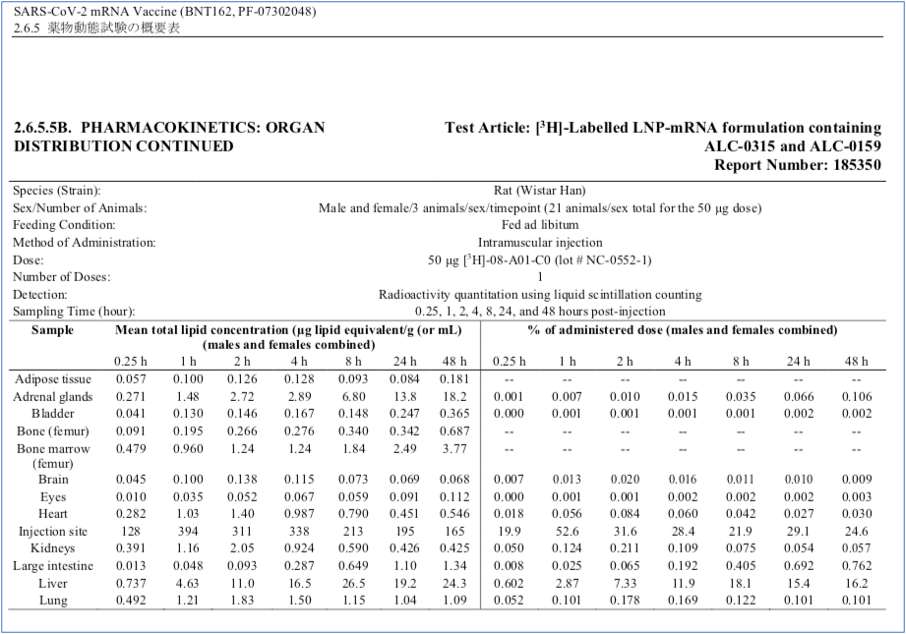
Although highest levels went to the spleen and liver, where high turnover of cells helps timely repair of any cytotoxic damage, the lipid-nanoparticle, and by implication the mRNA would as well, went to every organ, particularly the ovaries and adrenal glands but also the brain, eyes, heart, testes, uterus, pituitary gland, spinal cord, thymus, bone marrow.
Effectively the lipid-nanoparticle, and presumably its mRNA payload, distributes throughout the whole body. Spike proteins, that other research now shows are pro-thrombogenic (stimulate blood clotting) and pro-inflammatory, would be made in our cells everywhere.
Long-lasting mRNA
Messenger RNA is highly unstable in the natural form, so the mRNA that codes for spike protein in Moderna and Pfizer C19 vaccines has been stabilised by replacement of uridine with pseudouridine. This intervention has now been shown to make the synthetic mRNA excessively stable over a prolonged period. Research has found mRNA making spike proteins at 15 days, 28 days, and 60 days after the last jab. It is not clear when it stops.
When I’ve asked medical colleagues who are very much adherent to the ‘safe and effective’ narrative of these gene-based products, as to the pharmacokinetics of them – they seem to have a superficial knowledge. If they’re willing to hear about the biodistribution and long-life data, their confidence in the narrative clearly takes a pummelling. They’ve not known or thought about these implications.
Large numbers of mRNA and spike proteins
The pharmacokinetics are even more concerning when it is described that in a Pfizer dose there should be 30 micrograms of mRNA, and 100 micrograms in a Moderna dose and that leads to an estimated 30 or 40 Trillion mRNA, each producing many spike proteins and the human body has about 30 Trillion cells.
Apparent batch (lot) variability
The gene-based C19 vaccines were developed at ‘warp speed’ in 2020. This rushed development is a concern as mRNA technology, although around since developed by Dr Robert Malone and others in the 1980s, had never been used at commercial scale. This could be a reason for a reported variation in adverse events reports based on batch/lot of production.
This could explain why many people had no reaction to the C19 gene-based vaccines and a sizeable minority had significant to severe reactions.
A pharmacist with expertise in new product regulation, Maria Gutschi, explains from internal European Medicines Agency documents that data presented by Pfizer showed significant batch variability in amount and quality of mRNA. The upscaled mechanism to take laboratory based small quantities of mRNA to commercial quantities involves large vats of up to 900 litres of E.coli bacteria producing the mRNA from plasmid-DNA, which is just one potential reason for a degradation of quality and quantity. A more recent finding in the vials is residual plasmid-DNA which theoretically could make mRNA in the body for prolonged periods.
Another reason for variability of what’s in the vials is that the lipid-nanoparticle-mRNA complex requires extreme cold storage (minus 70o C) and any break in the ‘cold chain’ might render it ineffective – and harmless.
It would also explain how severe adverse reactions sometimes cluster in families and neighbourhoods. Former Australian Medical Association president and federal member of parliament, Dr Kerryn Phelps (cardiovascular) and her wife Jackie Stricker-Phelps (neurological) continue to suffer disabling conditions they attribute to the C19 vaccines. Daniel Shepard, a fit young man from Melbourne, and his girlfriend were both simultaneously admitted with post-Pfizer myocarditis to the same hospital in 2021.
Other concerns are that the lipid-nanoparticle might float to the top in vials, and that excessive shaking of vials can destroy the lipid-nanoparticle, which are further reasons why doses of mRNA might vary.
This should be grounds for a quality control investigation of the vials by the TGA and other investigators with the means.
Spike protein toxicity
If our cells produce a foreign protein/antigen it can cause our immune system to attack those cells, inducing autoimmune responses and inflammation that can be pathogenic and cause short term symptoms or longer-term disease. But the SARS-CoV-2 spike protein has been shown by some research to be toxic in its own right, when free from the rest of the virus. This is well summarised in a peer-reviewed paper by Italian pharmacologists called Understanding the pharmacology of COVID-19 mRNA vaccines: Playing dice with the spike? The literature on spike protein pathogenicity is accumulating.
Pharmacovigilance databases breaking records
Given the pharmacokinetic (where and how long the spike protein is made by the gene codes) and pharmacological (how the spike protein interacts with our cells) concerns, it is not surprising that adverse events are occurring. The number of adverse events for the gene-based C19 vaccines are more than 1½ times the adverse events tally for all vaccines combined over the decades long recording periods to the official pharmacovigilance databases (the US VAERS; UK Yellow Card; European Eudravigilance, World Health Organisation VigiAccess; and Australian TGA’s DAEN).
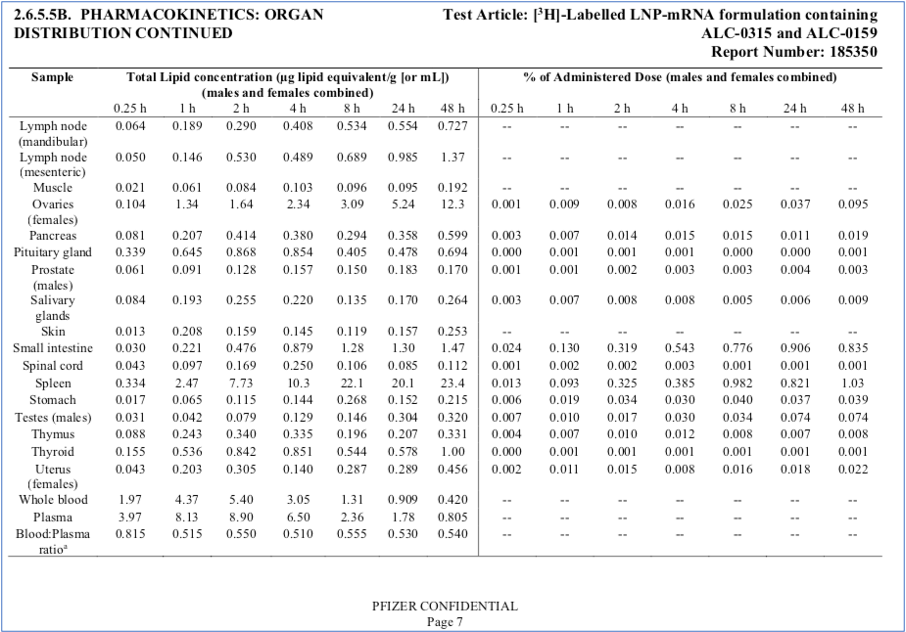
These databases have been used in the past to have medicines and vaccines recalled from the market. The anti-rheumatic analgesic, Vioxx, was on the market from 1999 to 2004, despite it being revealed in a Melbourne Federal Court case in 2009 that it’s manufacturer, Merck, knew it doubled the risk of cardiac arrests.
The FAERS (FDA’s drug adverse events reporting system, like the US Center for Disease Control (CDC)’s VAERS) reported death numbers of 6,636 when Vioxx was recalled after 5 years on the market. Later research published in The Lancet suggested the real number of deaths from Vioxx induced heart attacks in the USA alone to be between 88,000 and 144,000.
The website www.vaersanalysis.info provides comparisons of the adverse event reports of different vaccines and drugs up to the time of some prominent recalls of the products from the market due to safety risk (Figure 1). The data is up to the 17 March 2023.
Figure 1
The Vioxx data suggests the FDA’s adverse event database had an under-reporting factor of 13- to 21-fold. Yet, since the advent of the C19 vaccines, the health authorities who authorised the novel gene-based agents around the world have strenuously suggested the unprecedented adverse event reports, including deaths, are an over-reporting phenomenon. This new perspective contradicts historical use of these pharmacovigilance databases.
The Swine Flu vaccine in 1976 was pulled from the market after only 53 death reports out of 450 reports of Guillain Barre Syndrome (a progressive paralysis syndrome) after 45 million Americans vaccinated.
Despite historic evidence of under-reporting, as of 21 February 2023, the Australian TGA’s Database of Adverse Events Notifications (DAEN) had reports of 981 deaths from C19 vaccines, but the TGA recognises only 14 of them as proven (13 AstraZeneca, 1 Moderna). The tragic passing of an 18-year-old young woman was the Moderna C19 mRNA related death.
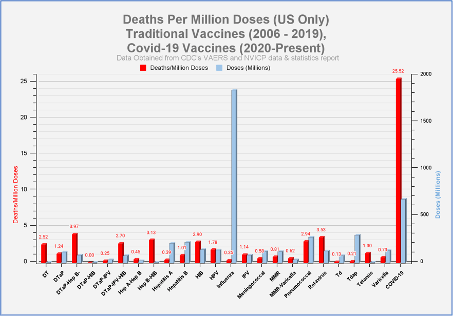
Comparing death reports on VAERS of all vaccines (the red bars being deaths/million doses) with the number of doses (the blue bars) paints a clear picture that the C19 vaccines have the highest death reports of any vaccine per dose – by a wide margin (Figure 2).
Figure 2
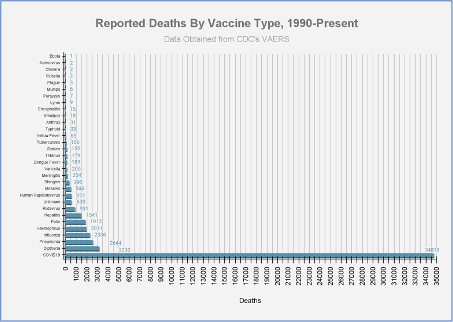
Another graph of VAERS data to February 2023 shows comparison of C19 vaccines’ deaths to all other vaccines in raw numbers over past 33 years (Figure 3).
Figure 3
It is odd that such official pharmacovigilance data is being dismissed by the media and authorities. I know from my doctoral research (chapter 4.6.4, p. 137-140) that similar pharmacovigilance data on deaths of children from antipsychotics detected by investigative journalists from USA Today and The New York Times researching the FAERS database, was later confirmed by peer-reviewed published research in the Journal of the American Medical Association (JAMA).
This pharmacovigilance data should be taken seriously.
Anecdotal data and case reports of vaccine injuries
I personally know or have met 10 fellow Qld Health employees who suffered serious adverse events, some with permanent symptoms or severe disability, from these C19 vaccines. Most suffered myocarditis/pericarditis, and other vaccine injuries were neurological. I also know others and have heard of many more.
One of my young colleagues suffered delirium and pericarditis following a first dose of AstraZeneca. She told me she felt “violated” by being forced to have a second injection which also made her very unwell although fortunately she did not get a recurrence of pericarditis. Many staff had to take sick leave following the C19 vaccines and said the reactions were worse than any other vaccine in their lives.
React19.org
Brianna Dressen is a US school teacher who volunteered for the AstraZeneca C19 vaccine clinical trial, suffered neurological adverse events and found her adverse events had been excluded from the trial data for publication in the New England Journal of Medicine. She joined with health professionals who also suffered C19 vaccine injuries to form a support and research community for those suffering harms from these products. The website collates lived experience, and lists over a thousand academic publications, regarding these adverse effects.
Statistical data on C19 vaccine morbidity
US CDC V-Safe survey
The US Center for Disease Control (CDC) ran a limited question survey called “V-Safe” about tolerability to the C19 vaccines. The results however were not voluntarily released by the CDC. An FOI and court suits that took 463 days was needed to get the CDC to release the data. The survey only listed minor adverse events in the tick boxes and did not record death data. It did ask whether the vaccine caused sick leave or need to attend for medical attention. Results like these don’t occur with normal vaccines:
Number of respondents to V-Safe survey = 10,108,273
Number unable to do normal activities = 3,353,110 (33.2%)
Of whom time off work/school = 1,344,330 (13.3%)
Number needing to seek medical attention = 782,913 (7.7%)
Phinancetechnologies.com
Edward Dowd is a former leading analyst for Wall Street firm Blackrock, he and two other Wall Street experts in statistics have compiled data from insurance companies and government statistics to show correlation of both increased disability claims and all-cause mortality with C19 vaccine rollout, particularly in younger working age adults. A book “Cause Unknown: The epidemic of sudden deaths in 2021 and 2022” by the same authors links this to many anecdotal reports of Sudden Adult Death Syndrome (SADS).
This team of Wall Street analysts calculate, based on US Bureau of Labor Statistics and V-Safe data combined with VAERS reports, a $148Billion cost in 2022 . That does not subtract any savings from C19 vaccines inducing lesser Covid-19 illness severity in people of older age with comorbidities, but it is likely much greater than the savings.
Myocarditis and ‘sudden adult death syndrome’
React19.org, under the heading “cardiac”, lists 133 peer-reviewed papers and case reports covering myocarditis, cardiomyopathy, myocardial infarction, cardiomyopathy, hypertension, postural othostatic tachycardia syndrome (POTS), tachycardia, and conduction disturbance
A recent study found free spike proteins in the blood of 16 adolescents and young adults who developed post-vaccination myocarditis, but not in 45 age matched post-vaccination controls without myocarditis.
The FDA recognised the risk for myocarditis and pericarditis from the C19 mRNA vaccines was real, particularly in younger males after the second dose, but judged it to still be rare, and cited a VAERS derived figure of 65 per million (6.5 per 100,000) and up to 200 per million (20 per 100,000) for adolescent boys
But the rate could be a hundred times that judging by a carefully conducted prospective study of adolescents after the second Pfizer dose in Thailand, that did serial ECGs, blood tests and Echocardiograms. Out of 301 teenagers, all with no prior cardiac history, 1 went to ICU with confirmed myocarditis and another six had subclinical myocarditis or pericarditis that might have been missed without the careful investigations. This equates to 2.3% or 23,000 per million.
Sudden Adult Death Syndrome (SADS) has only come to prominence since 2021. Things like ‘Climate Change’ are blamed – which is not to dismiss climate change – but how does that produce sudden deaths in healthy young people on mild or cold or even hot days that are barely a degree above historical records? A more plausible mechanism for delayed deaths is that myocarditis induces scar tissue that later leads to arrhythmogenic foci. Under stress or exercise these may trigger fatal ventricular fibrillation. In similar fashion, it is possible the pre-dawn circadian surge in catecholamines might explain the increasing anecdotes of relatively young people dying in their sleep.
The number of athletes dying while exerting themselves on the pitch/court has reportedly multiplied several-fold since 2021, although this has been fiercely contested by media fact-checkers. Which is countered by this article. Debating the data is integral to Science.
The risk is acknowledged after Covid-19 infection and this cardiology write up acknowledges it happens after C19 vaccine as well. However, this large study from Israel in 2020 predating the Israeli Pfizer rollout, found no statistical increase in myocarditis/pericarditis despite the early waves of Covid-19 in Israel. It is presumably harder for spike proteins to get to the heart when the virus is fought off by the immune system in the nose, throat, and respiratory mucosa.
Observation is the start of data assessment. I know several post C19 vaccine cases of myocarditis/pericarditis/heart attacks and have heard of many more through personal networks. This suggests the phenomenon is not ‘rare’. The tragic increased SADS cases correlate with C19 vaccines that are gene code insertions for spike proteins that for some people will cause thrombogenic and pro-inflammatory spike proteins to reach or be made in cells in the heart and blood vessels.
A systematic review of 50 autopsy studies of 548 patients who died with Covid-19 viral illness, median age 69, found mainly blood clots affecting the heart but almost no extensive myocarditis cases and a low rate of focal myocarditis, even though there was SARS-CoV-2 viral presence in 60% of the hearts of the deceased. This was a bit surprising but supports the Israeli study above. In contrast are the post-C19 vaccine autopsies done in Germany:
German autopsy case series
Two groups of German pathologists led by senior professors each did an autopsy case series of people (40 autopsies in Heidelberg; 25 in Reutlingen) who died shortly after C19 vaccination. Both groups reported finding evidence of causation by the C19 vaccine produced spike proteins. Prof Arne Burkhardt from Reutlingen shows slides with immunohistopathological staining finding what his group claims are spike proteins in the inflammation in organs responsible for the demise of the deceased, for example in the blood vessel wall in Figure 4.
Figure 4
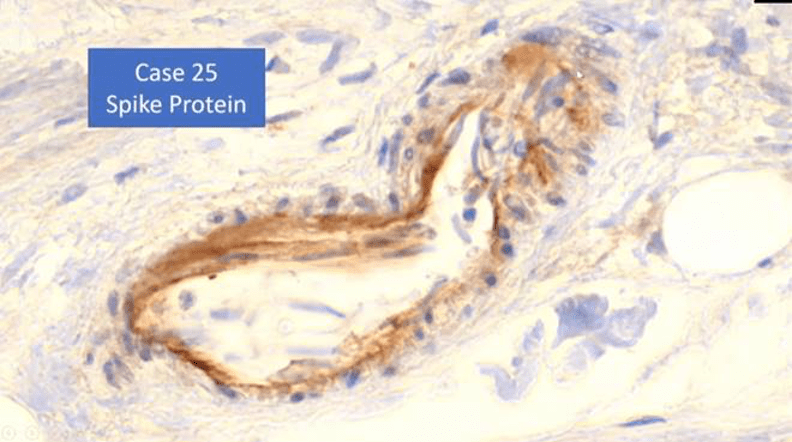
The translation from German accompanying this slide is:
“Yes, that is the finding that we have now been able to collect using special methods. This means that we are actually certain that in this case we can still detect this toxin in the vessel walls 122 days after the vaccination. It is also clear that this is the causal factor for this damage. What’s not clear to me at the moment is whether it’s just deposited there or whether these cells actually produce the spike protein, as they are told to do by the mRNA, so to speak.”
This sounds analogous to finding a smoking gun at the scene of the crime, only the last ‘shot’ was fired 122 days earlier.
Large literature of C19 vaccine harms
It might surprise many people including clinicians and health bureaucrats, but there is a large and growing academic literature on the harms of the C19 vaccines. In addition to the incomplete list at https://react19.org/1250-covid-vaccine-reports/ , there is the Twitter account of Dr John B, a senior clinical academic at a major Californian hospital who is highly published. He extracts the main points from hundreds of academic papers. I’ve communicated with him by email and to maintain his job he maintains anonymity, but his skill in reading the academic literature is evident from his tweets.
Limited efficacy of the C19 vaccines
It is now common knowledge that the C19 vaccines do very little if anything to stop infection and transmission. This was apparent in the Delta wave of 2021 and both Dr Fauci of the US NIAID and Dr Walensky of the US CDC admitted that viral loads in the noses of vaccinated and unvaccinated people were essentially equivalent. A study in Wisconsin suggested that a few vaccinated people might even be more likely to become super spreaders.
The rationale in the media for taking the C19 vaccines has shifted from protecting our grandparents to that of reducing severe Covid-19 illness. However, the current Omicron subvariants are proving to be mild, the virus mostly having lost the ability of the early strains to infect the lower lungs. For healthy people there is very little discernible benefit as shown in official data from the United Kingdom Health Security Agency (UKHSA) (Figure 5).
The number needed to vaccinate (NNV) is how many people need a vaccine to prevent one person needing to go to hospital, or for “severe hospitalisation” to need Oxygen therapy or ICU care. The NNV varies by age group and whether one has sufficient “at risk” comorbidities.
Figure 5
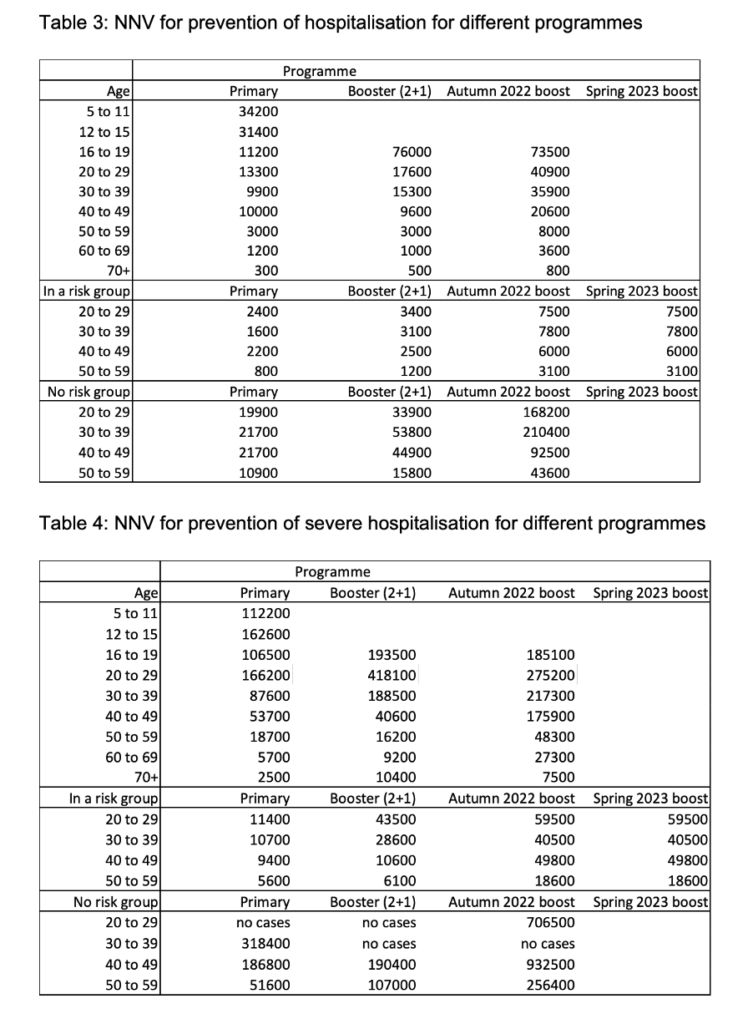
These numbers show a very low cost/benefit. For the current Omicron variants and current C19 boosters, 932,500 healthy people in their 40s would require C19 vaccination to prevent any requiring oxygen therapy or an ICU admission. Though – showing that individual personalised medicine is what matters – ‘only’ 18,600 people in their 50s with comorbidities would need a booster to prevent requirement for hospitalised oxygen therapy or ICU care.
Even for septuagenarians, the benefit does not outweigh the risk of serious adverse event of 1:800 from a Moderna or Pfizer C19 vaccine as calculated from the clinical trial data by Fraiman et al. (2022). Unfortunately, the UKHSA data did not include elderly at-risk where presumably the NNV would be much lower.
Lancet systematic review: Natural immunity at least as effective as vaccine immunity
A recent extensive systematic review and meta-analysis in The Lancet concluded that natural immunity post-infection with Covid-19 was at least as effective as vaccine immunity. Data showed it was generally longer lasting. The review was funded by the Bill & Melinda Gates Foundation.
Bill Gates stated publicly:
“Sadly, the virus itself, particularly, the variant called omicron, is a type of vaccine, that is, it creates both B-cell and T-cell immunity, and it’s done a better job getting out to the world population than we have with vaccines,” the Microsoft co-founder said.
“That means the chance of severe disease, which is mainly associated with being elderly and having obesity or diabetes, those risks are now dramatically reduced because of that infection, exposure.”
It is common sense as well as historically accepted medical wisdom, that natural immunity after infections is just as good as vaccine immunity. I am old enough to remember having my measles, mumps, rubella, and varicella (chicken pox) as infections, they all provided lifelong immunity. Rapidly evolving coronaviruses and influenza viruses cause recurrent illness, which is why annual immunisations for influenza lessen disease severity but don’t stop transmission and have never been mandated. In 2004 Dr Fauci acknowledged the superiority of naturally acquired immunity to influenza and there was no need to get a flu vaccine.
Here is a list of 162 studies on the benefits of natural immunity.
As natural immunity is as good as vaccine immunity, and probably longer lasting, why are thousands of Qld Health staff, most of whom have had Covid-19, excluded from returning to their jobs?
Risk/Benefit analysis and Medical Ethics
The study by Fraiman and colleagues looked at publicly available data from the Pfizer and Moderna mRNA C19 vaccine clinical trials published to the website clinicaltrials.gov that houses clinical trial data. This is only the data that the pharmaceutical company sponsors have permitted to be released. Although ethically they should release it all, as described above, clinicians, scientists, health bureaucrats and the public have to take this on trust, despite Big Pharma’s legally proven untrustworthy track record.
These are some of the internal pharmaceutical industry documents that shocked me beyond my own cognitive dissonance and denial 15 years ago. Pfizer puts commercial interests first in what data it will release (Figure 6) as does AstraZeneca (Figure 7).
Figure 6
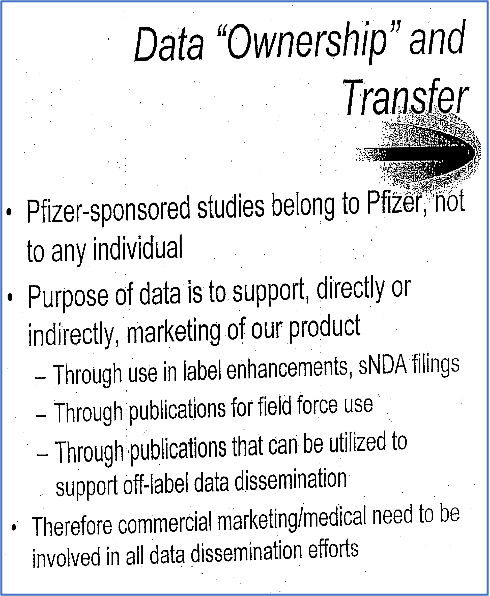
Figure 7
Even if the data posted to clinicaltrials.gov and published in the NEJM, was spun to look better than the raw data, Pfizer and Moderna still showed the risk of serious adverse events in excess of placebo was 10.1 per 10,000 people for Pfizer and 15.1 per 10,000 for Moderna. That is rare but equates to a Number Needed to Harm (NNH) of 1 in every 990 for Pfizer and 1 in every 662 for Moderna, which is interesting as Moderna gives about 4 times the dose of mRNA as Pfizer.
They average to 1:800 for both mRNA vaccines. That equates to 12,500 serious adverse events for every million doses. There’s been 65.5 million doses given in Australia to the end of March 2023. Based on the likely understated adverse events of the published clinical trials, that would equate to 818,750 serious adverse events among Australians by now.
Given the UKHSA data, both the risk/benefit and the cost/benefit to the health budget are deleterious, except possibly for elderly with comorbidities.
Medical Ethics is built on four pillars: Beneficence (the treatment must do good); Non-Maleficence (the treatment must not do harm, and certainly less harm than good); Autonomy (the patient has right to free informed consent and bodily autonomy); Justice (equitable treatment of all people is a human right).
It is not hard to see that the current C19 vaccine policy as embodied in the HED12/21 fails on all four counts. Benefit does not outweigh Risk. There is no possibility for autonomy, true informed consent and maintaining one’s job. The C19 vaccines are enriching Pfizer, Moderna and AstraZeneca while – at least now in 2023 – providing minimal value for money in terms of reducing Covid-19 illness burden, especially for healthy non-elderly people. That is $Billions being spent on these products while public health services are running major budget deficits after all the Covid measures, and services are likely to be cut as a result.
Justice also applies to the issue of fairness and treating people equally. The HED12/21 stipulated that all Qld Health staff must be up to date with their C19 booster doses and report their receiving a booster to their line managers within a week (Figure 8).
Figure 8 HED12/21 p. 3, section 8.1
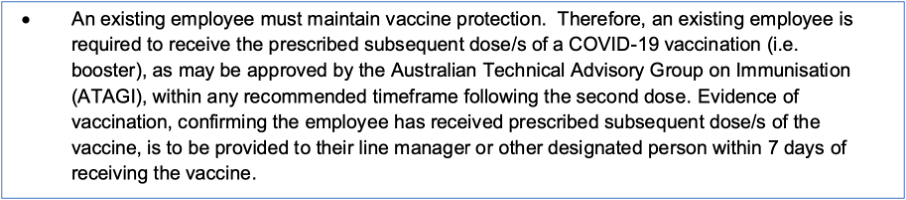
The recent ATAGI advice on boosters for people without risky comorbidities, shifted to “recommend” for only over-65-year-olds from 8 February 2023. The ATAGI advice is that not at increased risk 18 – 64-year-olds should “consider” a booster if it is over 6 months since the last C19 vaccine dose.
The recommendation was in place for all adults during 2022 when most Qld Health workers were therefore in breach of the strict wording of the HED12/21, based on these numbers obtained by Right to Information (RTI) from Qld Health (Figure 9):
Figure 9
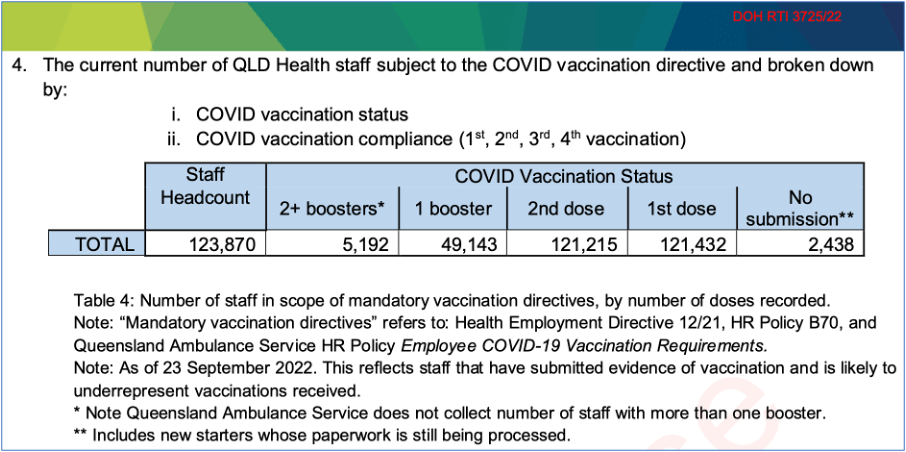
Qld Health responds that more staff got boosters than reported it to their line managers, nonetheless it appears that many thousands of currently employed Qld Health staff breached HED12/21. While I am not arguing my former colleagues should’ve got boosters, given the data presented here on risk/benefit and cost/benefit, this is a case of discrimination against the thousands of Qld Health staff who’ve been terminated from our jobs based on the HED12/21 rules.
Informed Consent
Australia has signed the United Nations International Covenant on Civil and Political Rights, which states: “no one shall be subjected without his free consent to medical or scientific experimentation.” (United Nations General Assembly, 1966). In addition, the Nuremberg Code on Medical Experimentation clearly states:
“A person involved should have legal capacity to give consent; they should be so situated as to be able to exercise free power of choice, without force, fraud, deceit, duress, over-reach or other ulterior form of constraint or coercion; they should have sufficient knowledge and comprehension of the subject matter involved to enable an enlightened decision.”
Furthermore, the Australian Immunisation Handbook states:
“For consent to be legally valid … It must be given voluntarily in the absence of undue pressure, coercion, or manipulation. … It can only be given after the potential risks and benefits of the relevant vaccine, risks of not having it and any alternative options have been explained to the individual. … The individual must have sufficient opportunity to seek further details or explanations about the vaccine or its administration.”
These conventions and protocols have standing in terms of human rights and codes of practice.
AHPRA confirms the right to speak based on Science
On the eve of the vaccine rollout in Australia on 9 March 2021, reflective of concern to protect the people from Covid-19, the Australian Health Practitioners Regulatory Authority (AHPRA) issued a position statement warning of disciplinary action for practitioners who “discouraged their patient or client from seeking vaccination”. This statement, and the warnings and deregistration of practitioners in the wake of it, closed down scientific debate even though the letter qualified that practitioners could “use their professional judgement and the best available evidence”.
However, in a 21 March 2022 letter responding to inquiry by Senator Gerard Rennick and solicitor Tony Nikolic, AHPRA further qualified the statement:
“The position statement does not prohibit, restrict or unduly influence practitioners from making any statements [about the C19 vaccinations] it simply requires those statements to be based in science and rely upon the best available evidence.”
However, this qualifying letter did not get much publicity. Health practitioners had been de-registered with a chilling effect on medical, public, and scientific discourse. Changing the discourse environment to a more open, transparent space for respectful, data-driven debate has been slow.
Pfizer-government contract secrecy, regulatory agency secrecy
There are events which reveal we do not have transparency to make fully informed choices and fully debate the Science.
The Pfizer contract with governments around the world is secret. Even from elected representatives of the people. Did you know that? Members of the European Parliament have tried unsuccessfully to obtain a readable copy of the Pfizer contract with the EU Commission for two years, and only managed to get a heavily redacted version.
The FDA refused to release the Pfizer clinical trial documents that it based its Emergency Use Authorisation (EUA) upon. When Public Health & Medical Professionals for Transparency (PHMPT) asked through a FOI request, the FDA declined and argued in a US court to be granted 55 years, and then 75 years, for time to redact and release the documents. Perhaps there would still be too many people vaccine injured in 2076, and 2096 would be safer?
Fortunately, the judge ruled against the FDA and 100,000s pages of Pfizer clinical trial documents were released during 2022 and are being examined by a team of over 3,000 volunteers including many medical academics. Findings show some anomalies around the 170 (8 Pfizer arm, 162 placebo arm) with positive PCR tests, out of the ~44,000 enrolled participants in the Pfizer clinical trial upon which the “safe and 95% effective” message was based.
Figure 10 shows the positive PCR tests for placebo participants (orange bars) and Pfizer C19 vaccine participants (blue bars) until the minimum cut-off figure of 164 cases is surpassed to provide a statistically acceptable result. The number of participants excluded from the trial is also shown in chronological order as well.
Figure 10
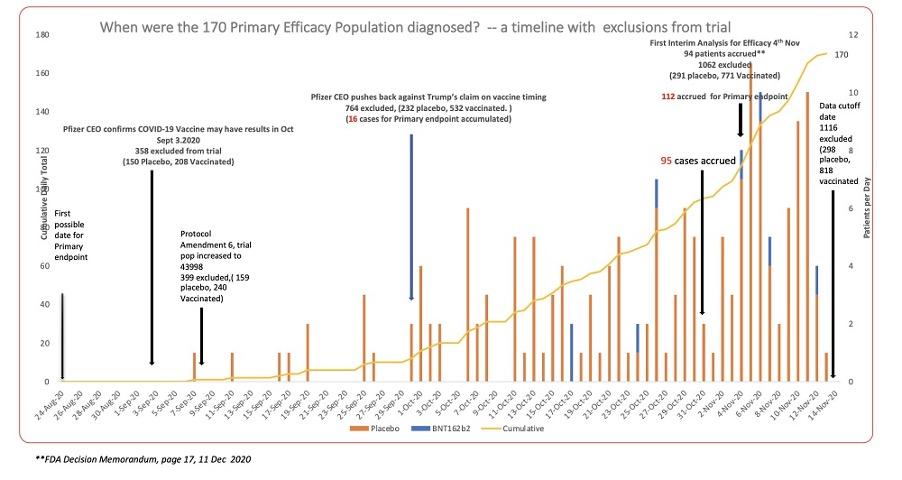
As few as 170 (8 Pfizer arm, 162 placebo arm) out of two arms, each with approx. 22,000 participants, is what the “95% efficacy” is based upon. But also 818 in the Pfizer arm and 298 in the placebo arm were excluded from the analysis up to this point. Why are 73% of exclusions from the Pfizer C19 vaccine arm of the study? If just a small number were PCR positive the efficacy results would have been far lower.
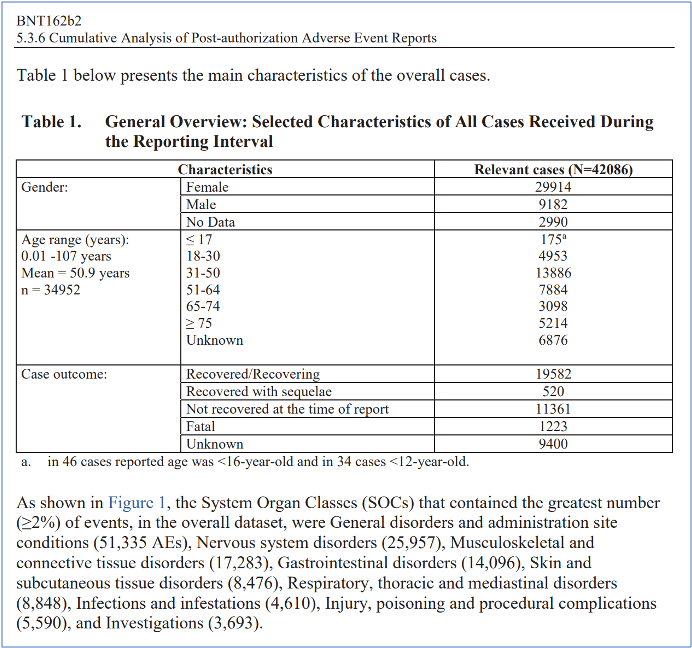
A Pfizer document submitted to the FDA early in 2021 was of pharmacovigilance reports of adverse events it collected from December 2020 public release to 28 February 2021. In those 10 weeks or so, 42,086 people reported adverse events of which many had not resolved and 1,223 were fatal (Figure 11).
Figure 11
Whistleblowers such as Pfizer clinical trial site director Brook Jackson report on the unblinding of the clinical trial during its conduction. So it would have been possible to shift a few score participants to obtain the desired result. After reading over 400 internal industry documents, I can say it would be consistent with past behaviour (as per Figures 7 & 8 above). Recall that those earlier Pfizer and AstraZeneca and other company documents were subpoenaed for criminal trials and released upon conviction of felonies.
Other whistleblowers: Brianna Dressen (neurological) in AstraZeneca trial, Maddie de Garay (neurological) and Augusto Roux (myopericarditis and liver inflammation) in Pfizer trial suffered major adverse events and were written out of the articles published in the New England Journal of Medicine (NEJM). The chief-editor of the NEJM was informed of the discrepancies. The chief-editor refused to have the peer-reviewed published papers (that are still cited as a scientific basis for the HED12/21) corrected and replied that the aggrieved clinical trial participants needed to contact the FDA.
The FDA appears to have shown where its loyalties lie. The FDA, CDC, TGA and other medicines regulatory agencies, as well as the WHO all receive most of their funding from the pharmaceutical industry as reported in the British Medical Journal.
FOI requests to the TGA reveal it accepted most of the data it based its provisional approval decision of the C19 vaccines on, based on trust of the FDA’s investigations and deliberations. The TGA redacts and restricts what it releases under FOI.
The Pfizer-Government contract has been leaked in Albania and some Latin American nations. It includes a clause (1.54) that some allege seeks to limit Government support of competitor products, by contracting governments to full purchase of Pfizer C19 vaccine vials even if other products are developed. If that were the case, could it explain why Australians are denied a range of non-genetic (and non-Western BigPharma) C19 vaccines that are approved in other countries? Given that Members of the European Parliament still cannot access the EU-Pfizer contract, questions remain.
Who is indemnified against complaints of C19 vaccine injuries?
The Pfizer contract contains clauses indemnifying the company against claims of vaccine injury from adverse effects. The Government takes on the cost of such claims. However, medical, nursing and pharmacy colleagues administering the C19 vaccines might want to familiarise themselves with this information.
Dominant narratives and human nature
Humans are a social mammalian species with group tribal dynamics deeply embedded into our psychology and group behaviour. Although we call ourselves Homo Sapiens Sapiens (wisest of wise hominids), we have evolved, like other herds, flocks, prides, packs, of mammals and birds, the tendency to follow the leader and follow orders. This is very important for survival, especially when the group is dealing with a threat.
The extent of authority bias and groupthink conformity was found to be extreme in the social experiments of psychologists Solomon Asch and Stanley Milgram. Both Asch and his student Milgram wanted to understand the psychology of Nazi Germany and other totalitarian regimes of the mid-20th Century. Human history shows that groupthink behaviour is not uncommon.
Groupthink is accentuated in the face of a threat – like an epidemic disease. In such situations a dominant authoritative narrative for the group to ‘think as one’ is a necessity to escape the danger. Any dissident views must be suppressed because consideration would delay urgency of action. This would explain the apparent instinctive tendency to side with authority and dismiss and marginalise dissident views and those who voice them.
Dominant narratives have a way of becoming set in stone as it were, particularly when authority structures vital to cohesive society have staked reputations on them. This time behavioural science, as in the UK ‘Nudge Unit’ was used to engender fear and conformity of behaviour in the population. Even if the motive is to help health, this raises ethical questions about autonomy. The subliminal nudges of the UK Nudge Unit have been exported to governments around the world.
But what if dissident views are right, or partly right? What if urgency of action can lead to mistakes and neglect of safety checks? All I ask is you reflect on the past 3 years and think whether some degree of groupthink has operated, and we still haven’t fully emerged from it?
Dr John Campbell, PhD
Dr John Campbell is a nurse educator with a BSc and MSc in biology and a PhD and decades of experience in educating nurses and health professionals. At the onset of the pandemic, he had 20,000 subscribers to his YouTube teaching channel. He now has 2,730,000 subscribers. His motto on a poster he presents in front of is “Follow the evidence – wherever it leads.”
For the first couple of years of the pandemic Dr Campbell scrupulously followed health authorities and the major prestigious journals like the New England Journal of Medicine. He usually ended his presentations exhorting his listeners to “for goodness’ sake, get vaccinated!” But like falling stage lights from the sky in front of Jim Carrey in The Truman Show movie (an analogy I like because I apply it to my own journey), Campbell’s videos became increasingly focused on the anomalous data of high rates of adverse events, statistically high increases in all-cause mortality correlating with highly vaccinated populations, Covid pandemic prolonged in more highly vaccinated countries, the complexities of immunology and risk induction of immune tolerance – such as his discussions with Australian immunology expert, Prof Robert Clancy (who I’ve become privileged to know), the efficacy of suppressed off-patent medications and related matters of conflicts of interest. Prof Clancy has published a series of articles on Covid-19 in Quadrant.
A persistent FOI request after many months has obtained a document showing the TGA had the Pfizer biodistribution data rat study in January 2021, before issuing the C19 vaccine provisional approvals. Dr John Campbell reports on it and discusses implications with Senator Rennick and Prof Clancy . Dr Campbell yesterday discusses a further FOI obtained TGA document.
Dr John Campbell sticks scrupulously to the “best available evidence” in the words of AHPRA. He has shown how sticking to the evidence and using rational critical reason to formulate and follow hypotheses can lead to shifts in understanding and conclusions. He was influenced by our innate human authority bias at the start but not stuck in groupthink. Therefore, he has been able to shift viewpoint as the data necessitated. His videos are well worth watching. Similar can be said for Dr Philip McMillan, and his Vejon Health YouTube channel for discussing the research evidence.
Other clinical academics with views that chime with those of Prof Robert Clancy AO, are Americans Dr Pierre Kory who has led a team of doctors to compile the following reviews of clinical trials and Covid-19 treatment protocols and Dr Peter McCullough, who I met on their recent speaking tour here. I also have got to know Dr Phillip Altman, Pharmacologist and Clinical Trial and Drug Regulatory Affairs Consultant with more than 40 years’ experience. He was a founder of the international association for such specialists. He has documented issues with the C19 vaccines in a document I helped to edit along with Prof Wendy Hoy AO. Dr Altman and I also collaborated with many clinicians, clinical academics, medical scientists, and lawyers on an open letter to the TGA, ATAGI and Federal Health Minister in March 2022. Questions were respectfully put, based on evidence. The questions still await answers.
Legal challenges require financial support
Our DAM Judicial Review against the PHD of the CHO that ran from April to September 2022, cost each of us around $20,000 in personal costs and we were grateful for the extra $115,000 raised through https://www.mightycause.com/story/0hug6f . At present only a third of that remains and we need support, particularly as the HED12/21 might be defended in a full court hearing and not dropped. In which case costs will be higher than last year.
There are many expert witnesses, with vastly more detailed data than presented in this blogpost of mine, that we could ask, to add to our list of 5 expert witnesses from last year’s action.
It would be good if an Australian court could see a full array of the evidence from both sides of this debate. Please donate at: https://www.mightycause.com/story/0hug6f.
Conclusion
If you have got this far, I sincerely thank you. I can’t claim to have interpreted all the information perfectly. A spirit of open-minded inquiry and respectful scientific debate will lead to more accurate understanding.
But I trust you can see there is a large amount of information for making an informed decision to decline rather than consent to receiving a genetic code for C19 spike protein in one’s body. Ask yourself – should anyone’s career and job be contingent on this? It’s not just health professionals, but police, military, firefighters, pilots, and many others who lost jobs. Especially with milder Omicron, no significant difference in infection and transmission and a top-level systematic review in The Lancet attesting to no benefit over natural immunity.
In medical school I remember reading a book of Martin Luther King Jr’s collected speeches & sermons. They were profound, moving, and inspiring. MLK said: Our lives begin to end the day we become silent about things that matter. I’ve spoken out because the above information matters.
[Thank you for reading Peter’s story, please support this action at the Supreme Court with a donation if you think it is important to have this story and perspective considered by our justices. More stories to come.]